Overview of hyperhidrosis symptoms and treatment (misspelled
hyperhydrosis) options. Sweating is necessary
to control body temperature during times of exercise and warm/hot
surroundings. Sweating is regulated by the sympathetic nervous
system. In 0.6 to 1.0% of the population, this system is revved-up
and works at a very high level causing sweating to occur at inappropriate
times in specific areas of the body. This condition is known
as hyperhidrosis.
Classification Causes of hyperhidrosis
can be primary or secondary
Regions of the body affected Scalp,
facial (face), palmar (hands), axillary (armpits), truncal (trunk),
plantar (feet
Primary or idiopathic hyperhidrosis Hyperhidrosis without a known cause. A more frequent condition
than secondary hyperhidrosis. Localized commonly in the hands,
armpits, scalp, face, and/or feet. Starts during childhood or
early adolesence, worsens during puberty, and then persists for
the rest of one's life. Nervousness and psychiatric disorders
are rarely the cause. The excessive sweating is very embarrassing
and social, professional, and intimate relationships are often
seriously affected.
Secondary hyperhidrosis Caused
by an underlying condition. Usually causes excess sweating of the
entire body, however. Some of these conditions are; endocrine
disorders such as hyperthyroidism, endocrine treatment for malignant
disease, menopause, obesity, psychiatric disorders, systemic malignant
disease.
Scalp or Head/Facial Hyperhidrosis
and Blushing Excessive
sweating of the scalp and face. Commonly associated with moderate
to severe facial blushing as well. This condition often causes
the individual to become self-conscious and to develop a low
self esteem.
Palmar or Hand Sweating Hyperhidrosis
Far and above the area of the body causing the most distressing
condition. The hands are used socially and professionally more
than any other part of the body. Excessively wet hands may
even limit the choice of one's profession. Avoiding social
contact is common for individuals with severe hyperhidrosis
palmaris. Patients notice not only that their hands feel very
wet all the time, but also feel cold. Some individuals have
a bluish-purplediscoloration of their hands as well.
Axillary or Armpit Hyperhidrosis Minimally Invasive! An option for underarm sweating treatment called Micro ETS Learn
More Sweating of the armpits causes large wet marks
and staining on the clothes. A strong body odor develops quickly which
can cause very negative emotional/psychological repercussions. Slightly
more common in females than males. The highest incidence occurs
with people of Asian and Jewish ancestry, but can affect all races.
Click Image
to Enlarge
Peeling skin, or sweat blisters, are an example of how excessively
sweaty hands can affect the skin and a person's confidence.
Truncal/Thigh or Torso/Leg Hyperhidrosis
Less frequent. May be associated with sweating of other areas of
the body.
Plantar or Foot Hyperhidrosis
Excessive sweating of the feet. Can be associated with hyperhidrosis
of other areas of the body.
Symptoms (Characteristics) Either
sudden onset or continuous sweating. Sweating
usually brought on by no apparent reason. Usually not aggravated
by exercise. Emotional stress, high ambient temperatures, and/or
gustatory stimuli are the most important aggravating factors. Hyperhidrosis
usually improves during the cold/cool months and worsens during
hot/warm months. Sweating usually stops during sleep. Hereditary
(25% of individuals with hyperhidrosis tend to have a family member
with symptoms as well).
Hyperhidrosis
Treatment Secondary hyperhidrosis is treated by first
addressing the underlying disorder. If a patient is on hormonal
therapy then administration of an anti-estrogen (ciproterone
acetate) can give relief to sweat attacks. Primary hyperhidrosis
patients and secondary hyperhidrosis patients experiencing moderate
to severe sweating not relieved otherwise may benefit from the
following alternative treatment modalities; Antiperspirants
(Drysol), Iontophoresis.
Medications (anti-cholinergics), Surgery.
Hyperhidrosis Surgery Known
as endoscopic thoracic sympathectomy (ETS),
is the treatment of choice for severe hyperhidrosis. Interruption
of nerve impulses to sweat glands of the palms, face, axillae
(armpits) by cutting or electrocautery is called "Thoracic
Sympathectomy". The ganglia (nerve junctions) which lead
to the sweat glands of the palms, axillae, scalp and face are
accessible through the chest (thoracic cavity) because they
travel along the side of the spine of the back.Using
a Micro Single Incision endoscopic technique, easy access to
this area requires only a single 1/12th inch incision per side.
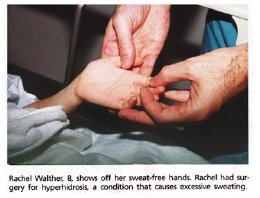
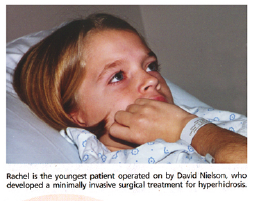
No Sweat - S.A. LIFE Surgery ends misery of wet palms, feet for 8-year-old girl.
Rachel, an 8 y/o female Wet Cold Hands Improved!
33 y/o female from Katy,TX tried 20+ years to make her wet/cold hands dry and warm.
16 y/o female from Ozar, wet hands become DRY and warm after Micro ETS
Calvin - Newfoundland travels to San Antonio for Micro ETS to stop Sweating Face/Scalp/Hands/Axillae
Katie travels from Utah to San Antonio to Stop her Sweating
In the past, a rib was removed or a large painful
incision was required between two ribs to provide access to this
area. Some surgeons today make three to four small incisions
when performing endoscopic thoracic sympathectomy. Dr.
Nielson has applied state-of-the-art technology to his
endoscopic technique and he only makes a single 1/12th inch
incision per side.
Precise cut of sympathetic nerve that is
much less painful
Nerve & ganglia are not removed
Surrounding tissue is not disturbed
T2 level cut only (T2/T3 for severe axillary
sweating)
Kuntz nerve cut
if present
Out-patient surgery (discharged the same day)
No sutures required
Rapid recovery
Operating time is short and postop
pain and discomfort minimal for patients who undergo this micro-incision
technique. Improvement is immediate
for scalp, facial, palmar, and axillary hyperhidrosis. Patients
leave the operating room with dry scalp, face, hands, axillae. Excessive
sweating of the whole body and/or trunk cannot be treated surgically.